PRIMARY OPEN ANGLE GLAUCOMA

INTRODUCTION:

Glaucoma
is characterized by the common characteristic feature of retinal ganglion cell
loss and optic nerve degeneration. There are different methods to classify
glaucomas. It can be categorized on the basis of etiology (Primary vs.
secondary), duration (Acute vs. chronic), and anatomy of the anterior chamber
angle (open vs. closed).
Primary
Open Angle Glaucoma (POAG) is defined as a chronic, slowly progressive,
optic neuropathy with characteristic patterns of optic nerve damage and visual field
loss. It is a subset of the glaucomas characterized by an open, normal appearing anterior chamber angle and raised intraocular pressure (IOP), with no other underlying disease.
World-wide
this type of glaucoma is the most prevalent. The global prevalence of glaucoma
among individuals in the 40-80 years age group is around 3.54%. POAG accounts
for 3.05% and primary angle closure glaucoma (PACG) 0.5% of the total
prevalence. According to the WHO, nearly 5.2 million people are blind
world-wide due to glaucoma. Of these, congenital glaucoma accounts for 200,000;
POAG 3 million and 2 million from PACG.
There
are many theories to explain the development of POAG. These include the
mechanical, vascular, biochemical, genetic and intraluminal pressure theories.
However, it is not known which etiology might be active in any particular
patient. It is often assumed that multiple mechanisms could be responsible for
glaucomatous damage in an individual.
CLINICAL
FEATURES:
POAG
is usually insidious in onset, slowly progressive, and painless. It is often a
bilateral, asymmetric disorder. The condition is called the “silent thief of
sight” as central visual acuity is relatively unaffected until late in the
disease. A number of risk factors for the development of POAG are known. These
include intra-ocular pressure, increasing age, race, decreased central corneal
thickness (CCT) and positive family history.
Intra-ocular
pressure:
Based
on population studies the normal mean IOP is 15.5 mmHg with a standard
deviation of 2.6 mmHg. This makes the range of mean normal IOP between 10-21
mmHg. However, it is known that IOP in the general population is skewed to the
right. A number of abnormalities in IOP measurement have been presented over
the last few years. The role of normal diurnal fluctuation of IOP has shown that
IOP measurements can be biased depending upon the time of measurement. This is
more obvious in glaucoma patients where IOP may fluctuate by more than 8-10
mmHg (compared to 5 mmHg in normal eyes).
Central
corneal thickness:
CCT
was found to be a powerful predictor for the development of POAG in OHTS. The
relative risk of POAG increased 81% for every 40 μ thinning of cornea. Both
OHTS and the European Glaucoma Prevention Study found that the risk of
developing POAG was greater in eyes with CCT <555 μ compared with eyes
having CCT of 588 μ or greater. Another study has reported that patients with
thinner corneas tend to have more severe glaucoma even on initial examination
and have a higher risk of progression. The actual IOP can be overestimated on
Goldman applanation tonometry in eyes with thicker corneas, whereas an
underestimation may happen in eyes with less than average CCT. Refractive
surgery can alter the corneal biomechanics and corneal thickness, thus
resulting in falsely low IOP readings. However, in the presence of corneal
edema IOP tends to be underestimated and is overestimated when measured over
corneal scars due to the increased rigidity of fibrous tissue.
Thicker
corneas resist indentation during tonometry leading to erroneously high IOP
readings. Conversely, in thin corneas the measured IOP can be falsely low. This
can affect the diagnosis of POAG. Corneal thickness may be measured
(pachymetry) by optical and ultrasonic methods.
Average
corneal thickness, determined by optical and ultrasonic pachymetry, is
approximately 530-545 µ in eyes without glaucoma. Central corneal thickness
(CCT) is increased in patients with ocular hypertension (OHT).
Other
confounding factors in IOP measurement are corneal steepness (Steeper corneas
resist indentation) and a mechanical factor called corneal hysteresis. Certain
new instruments such as dynamic contour tonometry and Ocular Response Analyzer
are able to overcome some of these factors.
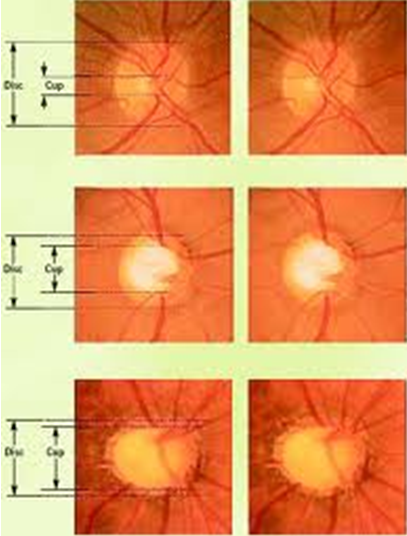
Optic
disc assessment and visual field loss:
Abnormal
cupping or an increase in the cup‑to‑disc ratio (CDR) is frequently associated
with glaucoma suspects. Stereoscopic evaluation of the optic discs has shown a
Gaussian distribution of the mean CDR at 0.4 with only an approximately 5%
normal population having CDRs of 0.7 or more. A difference of 0.2 between the
two eyes should be viewed with suspicion. Such a finding is present in only 1%
of the normal population.
It
is still not very clear whether structural changes (obvious on optic disc
assessment and other tests) develop earlier than functional changes (seen on
perimetric tests). However, careful periodic evaluation of the optic disc and
visual field is vital in the follow-up of glaucoma patients. Stereophotographs
of the optic discs are ideal to preserve the records of the patient for future
reference. However, computerized digital images or even hand drawings may
suffice, with the relevant details marked in the drawing. Stereophotographic
documentation or computerized imaging of the disc are useful as they enhance
the clinician's ability to detect subtle changes over time.
A
number of mechanical and vascular signs are found in glaucoma patients. These
include:
Mechanical signs
|
Vascular signs
|
Large
optic cup
|
Disc
hemorrhage
|
Asymmetrical
cups
|
Nasal
displacement of vessels
|
Progressive
enlargement of cup
|
Baring
of circumlinear vessels
|
Narrowing/notching
of rim
|
Tortuosity
of retinal vessels on
the
disc
|
Vertical
elongation of cup
|
|
RNFL
loss
|
|
Exposed
lamina cribrosa (laminar dot sign)
|
|
Peripapillary
atrophy
|
RNFL=
Retinal nerve fiber layer
Particular
attention should be paid to the neuroretinal rim (NRR). The rim is broadest
inferiorly among all quadrants, followed by the superior, nasal, and temporal
rims (ISNT‑rule). The loss of inferior or superior NRR leads to a vertical elongation
of the cup and loss of the ISNT‑rule leading to a suspicion of glaucoma. It
needs to be highlighted that ISNT rule is only applicable to normal sized
discs.
Visual
field loss should correlate with the appearance of the optic disc. Significant
discrepancies in the pattern of field loss and optic nerve damage warrant
additional investigation. As perimetry remains a highly subjective test, on an
average, 3 VF assessments should be done in the 1st year to detect an overall
change in mean deviation of 4 dB over 2 years in a patient with average VF
variability. Progressive VF loss is the hallmark sign which separates a true
pathology from a glaucoma suspect.
Gonioscopy:
Assessment
of anterior chamber angles is imperative for the diagnosis of POAG. The clinician
should be well versed with the procedure of gonioscopy. Angles which are more
than Grade 2 are regarded as open. If peripheral anterior synechiae are
present, the extent of PAS should be recorded.
Increasing
age:
In
a number of landmark studies increasing age was noted as a significant risk
factor. In the Baltimore Eye Study the risk of glaucoma increased significantly
in patients above 80 years of age. In the Collaborative Initial Glaucoma
Treatment Study (CIGTS) visual field defects were more common in patients above
60 years of age compared to those below 40 years.
Family
history:
The
lifetime risk for first-degree relatives of affected individuals to develop
open angle glaucoma is 22% when compared with a 2% risk in controls. it is
likely both monogenic and polygenic. Instances where a single gene causes
glaucoma (monogenic) have emerged (e.g., the myocilin and optineurin genes),
but in other instances glaucoma is much more likely the result of multiple
genes (polygenic).
Unique
susceptibility genes and genetic variants also likely play a significant role
in glaucoma.
TREATMENT:
Management
of open angle glaucoma has to be tailored for every patient. Initial treatment
usually consists of pharmacological therapy. Prostaglandin analogues and beta
blockers are the preferred agents to initiate treatment. Depending upon various
factors drugs can be changed or added. Compliance is an essential factor to be
considered when target IOP is not achieved. Some clinicians prefer to perform
laser procedures (Argon Laser Trabeculoplasty) or even implantation of glaucoma
drainage devices (GDDs) as initial procedures. However, usually GDDs are used
in advanced cases. Trabeculectomy or Minimally Invasive Glaucoma Surgery (MIGS)
can also be utilized in certain patients. Glaucoma filtering surgery is usually
performed in the situation of uncontrolled IOP despite maximally tolerable
medical therapy. MIGS is usually combined with cataract surgery. In case there
is poor visual potential and ocular discomfort (painful, blind eye) the eye may
be treated with cyclodestructive procedures. A number of laser and surgical
methods are available. These include diode laser cyclophotocoagulation,
micropulse-trans-scleral cyclophotocoagulation and endocyclophotocoagulation.
Surgical techniques such as cyclodialysis are not commonly in vogue now.
 |
| Progressive glaucomatous optic atrophy |




No comments:
Post a Comment