

INTRODUCTION:
Corneal abnormalities are known to affect tonometry measurements. These abnormalities can occur due to diseases or after surgical procedures such as keratoplasty or scleral buckling. A number of methods have been described to overcome them. In the Goldmann Applanation Tonometer (GAT), taking 3 readings and then taking a mean or taking the reading in one axis and then rotating the head by 900 have been suggested. Some instruments claim to offer better measurements of intra-ocular pressure (IOP) by overcoming corneal factors such as hysteresis. The Ocular Response Analyzer (ORA) is one such instrument. A recent advance is the dynamic contour tonometer.
The PASCAL Dynamic Contour Tonometer (DCT) from Ziemer is a slitlamp mounted tonometer which claims to provide true IOP, independent of interindividual variations in corneal properties and biomechanics confirmed with intracameral measurements. It also apparently offers the highest repeatability for a refined IOP and glaucoma progression analysis, and determines Ocular Pulse Amplitude (OPA), which has been correlated to glaucoma risk.


The DCT does not require fluorescein, only local anesthetic is instilled. The device is centered in the middle of cornea and the device advanced forward until the lever arm is upright. Fine adjustments are made through the slit-lamp such that the contact area (black rim) is centered nicely. The Q-indicator-tone indicates proper measurement of IOP. The device can be connected to wireless printer or PC and is EMR compatible. It also has automatic self calibration, therefore, no additional calibration steps are needed. The biggest advantage in the present scenario of COVID-19 pandemic is the low risk of cross infection due to sterile sensor caps.

Hartmut Kanngiesser, PhD, and Yves Robert,
MD, (at the Swiss Federal Institute of Technology and at the University
Hospital of Zurich, Switzerland, respectively) developed the theoretical basis
and the clinical proof of concept for a radically different methodology, which
they termed dynamic contour tonometry (DCT). Their device's contoured tonometer
tip has a concave surface, which touches but allows the cornea to assume a
shape (close to its steady-state shape). In such a state no tangential and
bending forces act within the area of the cornea touching the tip. If the apex
of the cornea is tension-free, the pressure acting on both of its sides (inside
and outside) must be exactly equal. The presence of a miniaturized piezoelectric
pressure sensor flush inside the surface contour of the tonometer's tip allows
practitioners to measure the “extra-ocular pressure” at the corneal apex in
order to obtain a direct reading of the IOP at the opposite side of the cornea.
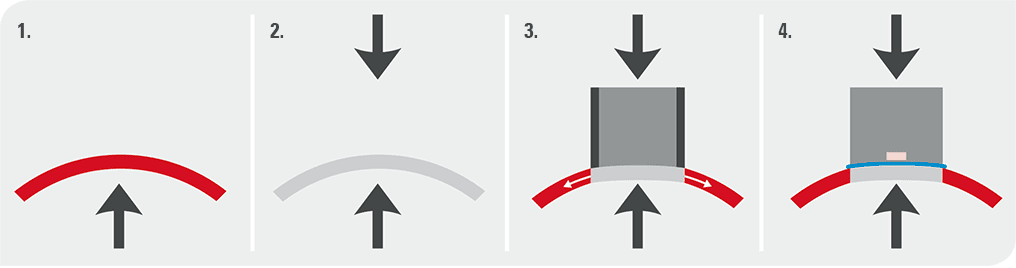

Due to IOP there is pressure on the cornea from the inside. However, due to the collagen matrix in the cornea, the corneal shape is maintained. The cornea is regarded as tension-free when the internal and external pressure across the cornea is equal. This is called Pascal’s Law. If the pressure in a small part of the cornea is equalized, the center becomes tension-free and flattens. This shape of the cornea is called the DCT-shape and the tonometer tip fits nicely in this shape. In such a tension-free state of the cornea the device measures true IOP, as if there is no cornea.
EFFECTIVENESS OF DCT:
Detailed mechanical analysis has demonstrated that variations in any corneal properties over a wide range of values does not influence this pressure measurement, and it showed that even the amount of appositional force applied to hold the tip in place does not affect the pressure reading.
Investigators analyzed tonometer data obtained with DCT, GAT, and pneumatonometry by plotting them against corneal thickness in healthy volunteers. Data from both GAT and pneumatonometry exhibited a significant correlation with corneal thickness; the measurements increased on average by 0.35 mm Hg per 10 µm of corneal thickness. In marked contrast, the DCT data were flat across the spectrum of corneal thickness readings, a finding that suggests that this tonometer alone functions independently of corneal thickness.
The chosen contour of the DCT tip will furnish correct measurements (defined as measurements with a systematic error of less than 0.5 mm Hg) for corneas with a radius of between approximately 5.5 and 9.2 mm and a corneal thickness ranging from 300 to 700 µm. Outside these limits, the systematic error will gradually increase. It is therefore important to note that some corneas will not satisfy the requirements for correct IOP measurements with DCT. Most nonpathologic corneas will be well within the scope of what DCT can handle correctly, however.
In a study performed in vivo, Andreas Boehm compared IOP in the anterior chamber with Pascal measurements prior to cataract surgery. (Boehm et al, 2008) This study demonstrated that DCT values were reliably within one millimeter of actual manometric IOP. In a more recent comparison between GAT and DCT IOP, Kotecha et al showed that DCT was more precise and reliable than GAT. (Kotecha et al, 2010).














