BIODEGRADABLE
COLLAGEN IMPLANT FOR TRABECULECTOMY
Guest author
SANA MAHREEN
Ajmal Khan Tibbiya College
Aligarh-India
INTRODUCTION
Trabeculectomy
currently remains the “gold standard” for filtration surgery.
A
disadvantage of this procedure is postoperative fibrosis and scarring, leading
to bleb failure and rise of intra-ocular pressure (IOP).
Concern
over postoperative scarring has led to the widespread intra- and post-operative
use of antifibrotic agents, particularly 5-Fluorouracil(5-FU) and Mitomycin C
(MMC). These agents, however, may bring an increased risk for chronic bleb
leaks, hypotony, blebitis and even endophthalmitis.
One
solution to this challenge may have its roots in the burgeoning field of “tissue
bioengineering”.
BIODEGRADABLE
COLLAGEN MATRIX IMPLANT
The
biodegradable collagen matrix (BCM) implant is being marketed, depending on the
country, as OlogenTM (Aeon Astron Corporation) or iGenTM
(Life Spring Biotech Company), both based in Taipei, Taiwan.

It
takes advantage of micro-technology and tissue bioengineering by having a
molecular structure that permits the formation of a spongy filtration bleb
without the use of antifibrotic agents.
The
implant is a 3D porous scaffold made of 1% collagen/C-6-S copolymer with a pore
size ranging from 20-200µ.
It
measures 4x7 mm and has a cylindrical shape, allowing for easy insertion and
manipulation during glaucoma surgery.
The
implant encourages the formation of a spongy meshwork of fibroblasts and
connective tissue in a controlled and organized pattern. It forces fibroblasts
and myofibroblasts to only grow into the pores, during the early postoperative
period and secrete connective tissue in the form of a loose matrix.
After
the polymer scaffold biodegrades, it leaves a milieu of organized fibroblasts,
myofibroblasts and extra-cellular matrix. This leads to a reduced scar
formation.
The
implant also maintains an elevated bleb while the healing process is underway.
In
trabeculectomy, early inflammation can lead to adhesion of the conjunctiva and
episcleral surface during the early postoperative phase.
SURGICAL
TECHNIQUE
A
conjunctival flap (limbus or fornix based) is created.
A
partial thickness scleral flap is then formed.
A
sharp blade is used to enter the anterior chamber at the base of the scleral
flap.
A
sclerostomy is created with a punch or en
bloc excision, after which the scleral flap is closed with two-to-four 10-0
nylon sutures.
The
BCM implant is then placed directly above the scleral flap and the conjunctiva
closed as per surgeon’s preference.

RESEARCH
ANIMAL
STUDIES:
Chen
et al performed trabeculectomy with the BCM implant in one eye of 17 rabbits
and standard trabeculectomy without anti-fibrotic agents in the fellow eye as
control.
For
the first 2 post-operative weeks IOP was similar in the two groups. Subsequently,
the IOP decreased in the implant group as the matrix dissolved. Conversely, the
IOP in the control group progressively elevated to post-operative levels.
Another
study was performed in 30 rabbits undergoing trabeculectomy with the implant
were compared with a control group of rabbits undergoing trabeculectomy without
it.
In
both groups, the conjunctiva was incompletely sutured to produce a wound leak.
Although the conjunctival defect sealed equally well in both groups, IOP was
significantly lower in the implant group after conjunctival healing was
complete.
HUMAN
STUDIES:
The
BCM implant is now available in Europe and Asia.
Chen
and Hsu reported the preliminary results of the experience in 12 patients. They
found a 64% reduction in IOP four months after surgery. The average number of
glaucoma medications also decreased from 2 to 0.3.
Ruokonen
et al. reported their experience in 17 patients with open angle glaucoma. IOP
improved from 30 to 14 mmHg within 3 months after surgery. The average number
of glaucoma medications required decreased from 3.3 to 0.2. Eleven eyes
developed bleb encapsulation with elevated IOP after 7 months. Of these some
responded well to needling and 2 required further surgery to control IOP.
Another
study reported the outcomes of 20 consecutive patients who underwent
trabeculectomy with implant placement. After 3 months, mean IOP decreased from
33.8 to 13.3 mmHg. All patients tolerated the implant well and no systemic
adverse-effects were noted.
Researchers
in China studied the effects of trabeculectomy with the implant versus
trabeculectomy without anti-fibrotics. The mean IOP was significantly lower in
the implant group after 6 months of follow-up. The risk of bleb failure was 30%
lower in the implant group.
The
BCM implant is also being used in cases of combined cataract extraction and
trabeculectomy. Grewel et al. studied 10 patients with POAG who were undergoing
combined phacoemulsification with trabeculectomy and implant placement. At 3
months post-operatively, mean IOP had improved from 20 to 9 mmHg and the mean
number of topical glaucoma medications needed reduced from 2.7 to 0.9.
CONCLUSION
The
BCM implant invokes the concepts of tissue bioengineering to promote successful
glaucoma filtration surgery. The implant is largely safe, easy to handle and
effective in reducing IOP without any side-effects as seen with anti-fibrotic
agents.

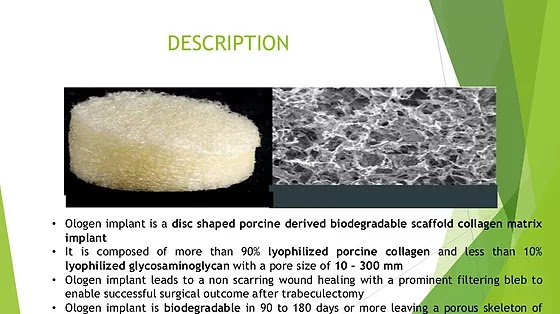
- The volume of ologen® Collagen Matrix creates a functional bleb which maintains a physiological barrier in the subconjunctival space that prevents subconjunctival scar formation.
- The porous structure of the collagen matrix induces random growth of the fibroblasts into the porous structure to prevent scar formation and to modulate the wound healing process.
- ologen® Collagen Matrix has a superior water-absorbing abilityand an excellent pliable strength. When ologen® Collagen Matrix absorbs aqueous humor, it works like a reservoir and creates a tamponading effect on the scleral flap, which along with the use of a loose suture on the scleral flap maintains a dynamic controlled drainage of the aqueous humor outflow. These properties further prevent scar formation in the trabdoor and intra-scleral space and reduce the chances of hypotony which may be seen in trabeculectomy with the applications of anti-metabolites adjuncts before ologen® Collagen Matrix can be applied.












