CLASSIFICATION OF GLAUCOMAS

The classification of glaucomas has seen a progressive change as
our understanding of this condition has evolved. The anatomic, gonioscopic,
biochemical, molecular and genetic basis for the classification of glaucomas
has been utilized, each having its own pros and cons. With the advent of new
instruments to diagnose glaucoma, classifications have also been created based
on the techniques utilized. Thus, the classifications of glaucoma include those based on:
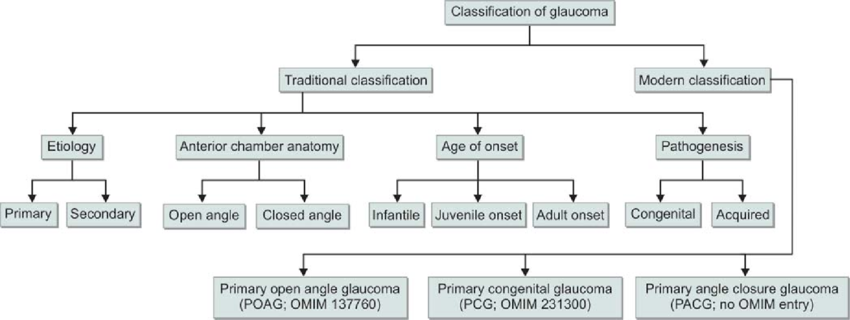
-Etiology
-Mechanism
-Staging
-Optic nerve appearance
-Visual field damage
-Standard HRT parameters by bagging classification trees
-Automated classification of glaucoma stages using higher order
cumulant features
-Texture features using neural networks
Unfortunately, none of the classifications have been
satisfactory in their attributes to describe glaucoma. This is not unexpected,
since there are different mechanisms of the disease and multifactorial
pathogenetic factors at work in different individuals. Presently, the
classification of glaucomas based on etiology and mechanism is still applied
in clinical practice, having stood the test of time over the years.
Etiologic Classification= This is based on the underlying disorder causing
alteration in aqueous inflow/outflow (Aqueous humor dynamics) or Retinal
Ganglion Cell (RGC)/Optic nerve damage.
Mechanistic Classification= This is based on specific alteration in the anterior
chamber (AC) angle that causes intra-ocular pressure (IOP) to rise.
These classifications have incorrectly been based on our focus
on elevated IOP as the major risk factor for the development of glaucoma,
excluding other factors such as vascular, genetic or biochemical mechanisms
among others.
CLASSIFICATION BASED ON ETIOLOGY
Based on the etiology, glaucomas have been divided into primary
and secondary. The primary glaucomas are assumed to have the initial events
leading to outflow obstruction and IOP elevation primarily in the AC angle or
conventional outflow pathway. These glaucomas are not associated with known
ocular or systemic disorders which could impede aqueous outflow. They are
usually bilateral and probably have a genetic basis. From a therapeutic
standpoint it is essential to differentiate open angle glaucoma from
closed-angle glaucoma.
On the other hand, secondary glaucomas are regarded as such
because of a “partial understanding of the underlying, predisposing ocular or
systemic events” [Bruce Shields]. These are usually asymmetric or unilateral.
While some may have a genetic basis, others are acquired. As the concepts
regarding the underlying causes of the glaucomas continue to develop, the
primary and secondary classifications have become increasingly artificial and
inadequate.
Classification of childhood glaucomas, especially those
associated with developmental anomalies of the anterior chamber angle have been
dogged by overlapping and variably defined nomenclatures which frequently
denotes the age of onset rather than the underlying mechanism for the glaucoma.
Bruce Shields has recommended replacing traditional concepts with a new scheme that provides a “better working foundation for the concepts of mechanism, diagnosis and therapy that will shape the management of glaucomas for the foreseeable future”. He has classified glaucomas based on staging. According to him, glaucomas can be considered to consist of 5 stages:
Bruce Shields has recommended replacing traditional concepts with a new scheme that provides a “better working foundation for the concepts of mechanism, diagnosis and therapy that will shape the management of glaucomas for the foreseeable future”. He has classified glaucomas based on staging. According to him, glaucomas can be considered to consist of 5 stages:
Stage I: Initiating events
Stage II: Structural alterations
Stage III: Functional alterations
Stage IV: RGC and ON damage
Stage V: Visual loss

The initiating events (Stage I) are speculated to have a genetic
basis. Structural changes may start occurring in the RGCs or optic nerve head (ONH),
as a result of alterations in proteins in these regions. These structural
alterations (Stage II) could be subtle tissue changes in the blood vessels
supplying the ONH or in supportive elements of the lamina cribrosa. Or they
could act through mechanisms as yet to be understood. Structural changes may
lead to functional alterations (Stage III) such as reduced axonal conduction,
vascular perfusion to axons in the ONH or a progressive deformity of the lamina
cribrosa that may lead (alone or in conjunction with a relative IOP elevation)
to glaucomatous optic neuropathy (Stage IV), which gets reflected in subsequent
VF changes (Stage V).
Traditionally, glaucomas have been divided into open and closed
angle.
Chronic open angle glaucoma: This is characterized by optic
nerve damage in an eye which does not have evidence of angle closure on
gonioscopy and there is no identifiable secondary cause. Apparently
inherited susceptibilities lead to increased resistance to aqueous outflow and higher
vulnerability of the ONH to the level of IOP.
Pupillary block glaucoma: Primary Angle Closure includes asymptomatic
individuals with occludable angles who have not had an acute attack, as well as
those who had an attack which resolved spontaneously or with treatment prior to
the development of any detectable nerve damage. Primary Angle Closure Disease
(PACD) has been classified by the International Society for Geographical and
Epidemiological Ophthalmology (ISGEO) into:
(1) Primary Angle Closure Suspect (PACS): Such eyes have
iridotrabecular contact for atleast 2700 and normal IOP, ONH and
VFs.
(2) Primary Angle Closure (PAC): There is iridotrabecular
contact for atleast 2700 and raised IOP and/or peripheral anterior
synechiae (PAS), but with normal ONH and VFs.
(3) Primary Angle Closure Glaucoma (PACG): There is PAC with
evidence of glaucomatous damage in the ONH or VFs.
(4) Acute Angle Closure Crisis: There is periocular or ocular
pain, often accompanied by headache, nausea or vomiting, IOP >21 mmHg, circumcorneal
congestion, corneal edema, mid-dilated pupil and shallow anterior chamber.
Developmental anomalies of AC Angles:
These represent incomplete development of structures in the
conventional aqueous outflow pathway. These anomalies could be inherited or
acquired during intra-uterine life and lead to elevation of IOP. In some cases
the developmental anomaly is not associated with primary or systemic etiologies
and regarded as primary.
Pediatric glaucomas have been classified into the following
categories:
(1) Primary Congenital Glaucoma (PCG): Primary congenital
glaucoma that occurs at or shortly after birth or glaucoma of any etiology that
occurs in the same time frame.
(2) Primary Infantile Glaucoma: It is genetically identical to
PCG but presents 1-2 months after birth.
(3) Juvenile Open Angle Glaucoma: There is no ocular
enlargement; absent congenital ocular anomalies or syndromes; Open, normal
appearing angles; meets the glaucoma definition.
(4) Developmental Glaucoma: This term has been used as a giant
waste basket for nearly all childhood glaucomas that are not acquired immediately
after birth.
Glaucomas associated with other ocular disorders
This class includes those glaucomas in which the initiating
event is an abnormality of the ocular structures such as corneal endothelium,
iris, ciliary body, lens, vitreous, retina and so on. Or the initiating event
is a definite second ocular pathology such as tumor, hemorrhage, inflammation
and so on. Secondary glaucomas are properly considered to represent those eyes
in which a second form of ocular pathology has caused IOP to rise above the
normal range with consequent ON damage. The second ocular pathological
processes causing optic neuropathy may include=
i.
Neovascularization
ii.
Uveitic conditions
iii.
Trauma
iv.
Lens-related
CLASSIFICATION BASED ON MECHANISM
Elevated IOP is the major risk factor for the development of
glaucoma. However, the concept that statistically raised IOP is a defining
characteristic of glaucoma has been almost universally discarded. A
disadvantage of this mechanistic system is that it ignores the causes unrelated
to IOP. Also, many of the glaucomas have more than one mechanism of outflow
obstruction at different times in the course of disease. As a result some of
the glaucomas must be classified under more than one mechanistic heading. On
the plus side, the advantage of this classification is that our understanding
of the mechanisms of aqueous outflow obstruction is usually more complete than
our knowledge of initiating events. An understanding of the mechanism that
leads to aqueous outflow obstruction is important in developing a rationale for
controlling the IOP in each form of glaucoma.

Mechanisms of Open Angle Glaucoma=
The elements obstructing aqueous outflow may be located on the
anterior chamber side of the trabecular meshwork [TM] (pretrabecular
mechanisms); in the TM (trabecular mechanisms) or distal to the meshwork, in
the Schlemm’s canal or further along the aqueous drainage system (post trabecular
mechanisms).
Angle closure glaucoma mechanisms=
Angle closure mechanisms are the ones which cause apposition of
the peripheral iris to the TM or peripheral cornea. The peripheral iris may be
pulled (anterior mechanisms) or pushed (posterior mechanisms) into this
position. In anterior mechanisms usually a contracting membrane in front of the
iris pulls the iris towards the TM/peripheral cornea. It can also be caused by
consolidation of inflammatory products in this area.
In posterior mechanisms pressure behind the iris, lens or
vitreous causes the peripheral iris to be pushed into the anterior chamber
angle. These mechanisms can occur with or without pupillary block. Pupillary
block variants include pupillary block glaucoma in which there is apposition of
the mid-periphery of the iris and the lens, thus blocking the egress of aqueous
anteriorly through the pupil. The peripheral iris balloons in the form of “iris
bombe”. The functional apposition in these patients is due to a genetically
influenced configuration of the anterior segment of the eye. Such appositions
may also be seen in lens-induced mechanisms such as phacomorphic glaucoma or
ectopia lentis. Pupillary block can also occur from posterior synechiae. The “pushing”
mechanisms can also occur without pupillary block such as ciliary block
(malignant glaucoma), lens induced, forward shift of vitreous following lens
removal, intraocular tumors, cysts of uveal tract, retrolenticular tissue
contraction as in retinopathy of prematurity or persistent fetal vasculature.
Developmental anomalies of the AC Angles=
These represent incomplete development of structures in the
conventional aqueous outflow pathway. Examples of these include: congenital
glaucoma, Axenfeld-Reiger syndrome, Peter anomaly and iridocorneal adhesions.