FUCHS UVEITIS SYNDROME (FUS)

Fuchs described the condition in 1906. The clinical features comprised of: mild anterior uveitis; heterochromia; cataracts; and occasional glaucoma.
A similar condition was
previously described by Lawrence in 1843.
Also known as: Fuchs
Heterochromic Iridocyclitis; Fuchs Heterochromic Cyclitis; or Fuchs
Heterochromic Uveitis.
Usually unilateral.
Typical age of onset: 3rd-4th
decades of life.
Male: Female ratio is same.
The International Uveitis Study
Group describes FUS as: A chronic, unilateral, nongranulomatous inflammation,
mainly involving the anterior uvea, insidious in onset, low grade in activity,
affecting both genders equally, preponderance in those between 20-45 years old,
unresponsive to corticosteroid therapy, absence of systemic disorders and
generally with a good prognosis except for the development of cataract and
glaucoma.
However, 7.8-10% patients have
bilateral disease.
Etiologic theories: Likely a true
inflammation of immunologic origin, although no clear HLA association has been
described. It is possibly related to depression of suppressor T-cell activity.
Autoantibodies against corneal epithelium have been reported in almost 90%
cases. The condition was also reported in a father-son duo afflicted with
retinitis pigmentosa. A few cases with associated congenital Horner’s syndrome
have been reported. Clinical association with Toxoplasmosis, due to
chorioretinal scars and sarcoidosis has been suggested, but no clear evidence
is available so far. Chronic rubella infection is also reported to be
associated with FUS. Adrenergic denervation and sympathetic paralysis suggested
as patho-genetic mechanisms as well.
Uveitis is generally mild.
Patients may have a single episode with a protracted course. Although, the
condition may appear intermittent initially.
Characteristic fine stellate KPs
are usually seen in the lower half of cornea (occasionally involve the upper
half).
Iris has extensive stromal
atrophy. Transillumination of the iris shows a characteristic faint, uniform
translucence. (Translucency of surrounding ocular coats also reported).
Prior to the development of heterochromia,
iris changes may occur in the form of smoothening of the stroma and loss of
corrugations seen in a normal iris.
Heterochromia of the iris is
variable and an inconsistent feature. It is more obvious in blue eyes and
subtle or absent in dark irides due to equal pigmentation of the anterior and
posterior layers. In some patients the anterior layer is lost and a heavily
pigmented posterior layer becomes visible. This gives rise to a darker
appearance of the iris (Reversed Heterochromia). In some, especially bilateral
cases, heterochromia is absent.
Nodules are often present on the pupillary borders (similar to Koeppe nodules), though they may occur on the iris surface (Busacca nodules). The nodules in FUS are typically small and translucent. Small, refractile iris crystals are also typically seen (They represent Russell bodies and can occur in other uveitic conditions). The finding of unilateral nodules in dark individuals is especially useful, as the heterochromia is less apparent in these individuals.
 |
| Iris heterochromia (Left eye) |
Nodules are often present on the pupillary borders (similar to Koeppe nodules), though they may occur on the iris surface (Busacca nodules). The nodules in FUS are typically small and translucent. Small, refractile iris crystals are also typically seen (They represent Russell bodies and can occur in other uveitic conditions). The finding of unilateral nodules in dark individuals is especially useful, as the heterochromia is less apparent in these individuals.
 |
| Koeppe nodules |
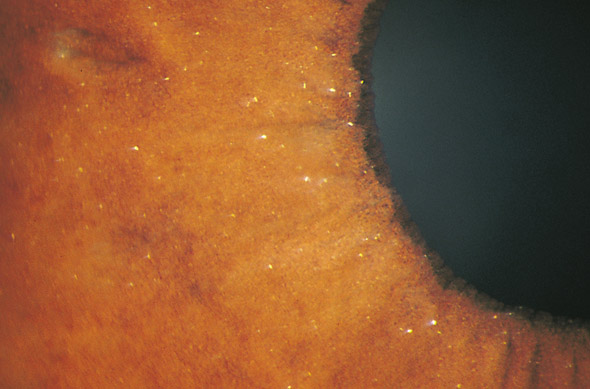 |
| Iris crystals |
The anterior chamber angle is
open and characteristically free of synechiae. Fine, branching, unsheathed,
meandering vessels are present in the angle, often extending upto the trabecular
meshwork. These vessels often give rise to filiform hemorrhages. These fine
vessels may bleed spontaneously or during Tonometry, gonioscopy, mydriasis or
surgery. These hemorrhages/bleeds are not associated with fibrosis or secondary
angle closure glaucoma.
Anterior segment neovascularization may occur in the absence of retinal ischemia. This is also possible in chronic uveitic conditions and iris melanoma.
 |
| Vessels in the angle |
Anterior segment neovascularization may occur in the absence of retinal ischemia. This is also possible in chronic uveitic conditions and iris melanoma.
Vitreous cells are common. They can
be dust-like to stringy or membranous veils.
Cataracts are quite frequent to
develop during the course of the disease. They start as posterior subcapsular
cataracts and rapidly progress to mature or hypermature stages. Surgery for
cataracts may require synechialysis and complicated with postoperative marked
anterior uveitis, corneal edema, hyphema, raised IOP and cystoid macular edema.
Patients should be covered with peri-operative corticosteroids. Visual prognosis
is usually good.
Raised intra-ocular pressure (IOP) in FUS is not as
common as in PSS. It may occur as a serious complication in late stages. The
mechanism for the elevated IOP is assumed to be increased outflow resistance at
the level of the trabecular meshwork. The elevated IOP typically persists after
resolution of the uveitis.
IOP does not respond well to corticosteroids.
Occasional and short term therapy can be used to control symptomatic
exacerbations. Long term steroids are ineffective and promote glaucoma/cataract
formation.
A steroid trial may also help to
differentiate FUS from other conditions, such as Posner Schlossman Syndrome and
other acute uveitic conditions with trabeculitis, which respond well to
steroids.
IOP control can be attempted medically,
failing which surgical management is required. Laser trabeculoplasty should be
avoided due to the inflammatory nature of the condition.




No comments:
Post a Comment